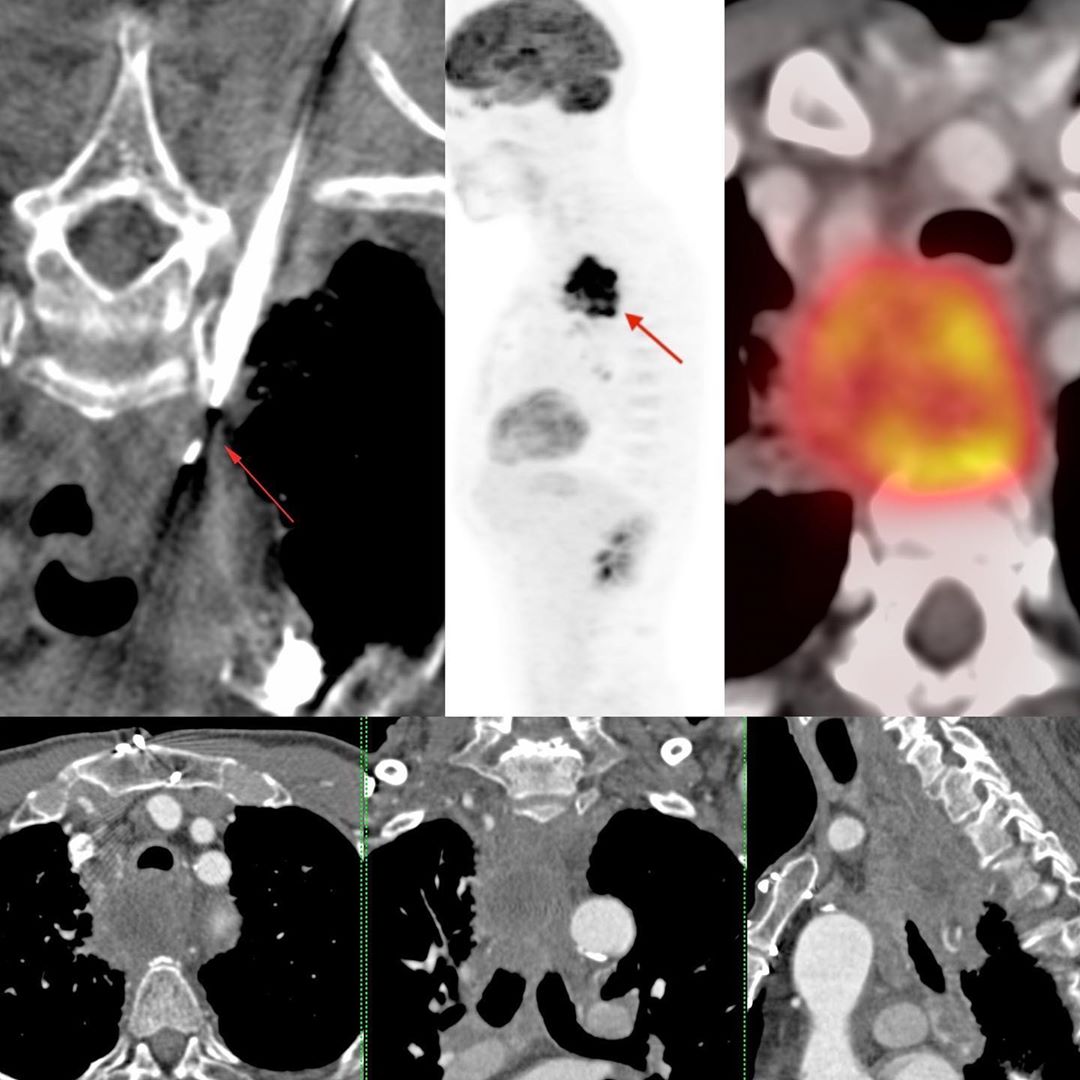
This 65-years old male smoker presented with dyspnea and dysphagia. He had a large necrotic mass in the retro-tracheal mediastinum. I don’t now remember the esophagoscopy findings, but either the lumen was not passable or it was normal. But it didn’t seem to be of esophageal origin.
In the prone position, it was easy to find an extra-pleural route from the right, after injection a combination of saline and lignocaine and then using a 20G coaxial biopsy gun. The diagnosis was poorly differentiated squamous cell carcinoma.
The PET was done subsequently and showed further necrosis and progression. I don’t have a further follow-up, but I still think this was of esophageal origin, perhaps exophytic or a primary mediastinal bronchogenic carcinoma in a smoker.
We don’t always need to biopsy with a scope. There is a lot we can do with CT scan guided biopsies.
Simple Extrapleural Approach – Posterior Mediastinal Squamous Cell Carcinoma
Blogs
Latest From Gallery





